The healthcare ecosystem is increasingly looking at an integrated approach to address wellbeing and health by partnering with community-based organizations (CBOs). This can make for a powerful, ‘dynamic duo’, that addresses whole-person care. But CBOs have traditionally been siloed from the healthcare ecosystem, creating a steep learning curve for those wishing to build business acumen and know-how for creating real partnerships (with real dollars attached) with healthcare.
In order for CBOs to capitalize on the opportunities available, it’s important to understand the trends and policy changes that are driving this push for integration. What’s motivating these partnerships from the healthcare perspective, what are they looking for in terms of partnership, and how can CBOs prepare? The short answer to the last question: social entrepreneurship.
Below is a summary from the webinar presented by Sharon Williams on this topic.
How healthcare reform impacts CBOs
“It is all about the Benjamins, baby!!”
The first thing to be aware of is the financial incentives driving the changes in healthcare and what is pushing changes in quality improvement, including the drive to contract with CBOs. Here are just a couple of the drivers.
- Affordable Care Act: The passing of the Affordable Care Act marked a shift in the delivery of care from a fee-for-service, quantity based system to a value-based care model, quality based system. This shift was meant to tie value and outcomes to how healthcare providers get paid. An example is hospital readmission reduction programs, which created penalties for readmissions to the hospital post-discharge. This created a strong financial incentive for hospitals to take a vested interest in what happens in the home and community setting once a patient leaves the hospital, an area of expertise among community-based organizations.
- Medicare Advantage (MA) Expansion: Through the introduction of the Chronic Care Act, Medicare Advantage was able to provide supplemental benefits not traditionally included in Medicare in order to support people living with chronic conditions. Supporting people living with chronic conditions is not just about clinical treatment. In order to address this oversight in the medical model, Medicare Advantage allows for Special Supplemental Benefits for the Chronically Ill, including services like the ones CBOs have traditionally offered, such as respite and caregiver support or nutrition services.
- The healthcare balancing act: There are many other drivers at play and the healthcare system is constantly balancing many demands around performance standards, quality measures, contractual requirements, member satisfaction, DEI, and others. Contractual requirements, for example, for healthcare systems to consider language competency might mean they look externally to CBOs to bolster accessibility. Member experience might necessarily encompass cultural competency because if your providers can’t relate to the unique needs of the population, the efficacy of that health system is compromised. These are all areas where CBOs can support the success of overall care delivery.
What are the objectives of healthcare integration
So what are some of the goals and objectives of integrating the delivery of care with social determinants of health, given the financial incentives brought along by healthcare reform in the past few decades. Here are just a few examples:
- Reduce preventable hospital admission/readmissions
- Reduce preventable Emergency Room utilization and avoidable costs
- Postpone institutional care/increase community-based care
- Reduce overall cost of care
- Improve consumer experience and engagement
- Person centered care planning
Bridging the gap between healthcare and community-based organizations
One population in particular to make note of in discussion about integration is the dual eligible population. These are individuals who are dually eligible for Medicare and Medicaid. Dual eligibles are a sweet spot for reform because of the high costs and the overrepresentation in spending associated with this population, and they have unique needs that often go beyond clinical care. Many CBOs are already serving dual eligibles, a group of about 13 million currently and quickly growing.
Sustainability for CBOs into the next several decades absolutely means adapting to the changing environment, expanding the current consumer base, and diversifying revenue streams to look beyond Older Americans Act funding and Medicaid waiver dollars. CBOs must become social entrepreneurs who think of themselves as innovators capitalizing on new business opportunities within the healthcare ecosystem.
Why are these relationships between healthcare and CBOs so important?
For the healthcare ecosystem:
- Emphasis on integration of healthcare and social services through healthcare reform
- Recognition of value of services addressing SDoH and community living services that impact health outcomes
- Drive toward value-based care
For CBOs:
- Increasing recognition of their own value in healthcare delivery and quality outcomes
- Need for sustainable revenue sources
What is healthcare seeking from CBOs?
What are healthcare players looking for when they consider working with a CBO partner? There are many things to consider, including the types of services they’re looking for and the readiness of that partner to take on contractual obligations and be a high-quality partner.
Services:
First and foremost, does a CBO deliver the service they need? Here are some services worth considering.
- Complementary / wrap around services / supports: Healthcare providers are not typically going into patients’ homes, but CBOs are. The case managers, meal delivery drivers, volunteers, etc are providing valuable ‘wrap-around’ care that complements the clinical side of care.
- Community engagement and hard-to-reach consumers: The four walls of the hospital might limit the clinical delivery of care, where CBOs have built trust within communities to engage on important public health discussions, especially with harder-to-reach consumers who may have been traditionally unengaged with the healthcare system.
- Caregiver support: A doctor might write someone a prescription but they are not always asking about that person’s caregiver, who is playing a critical role in keeping someone healthy and well. CBOs that provide respite care, caregiver education, or other supports help caregivers in their ability and readiness to support patients with complex needs.
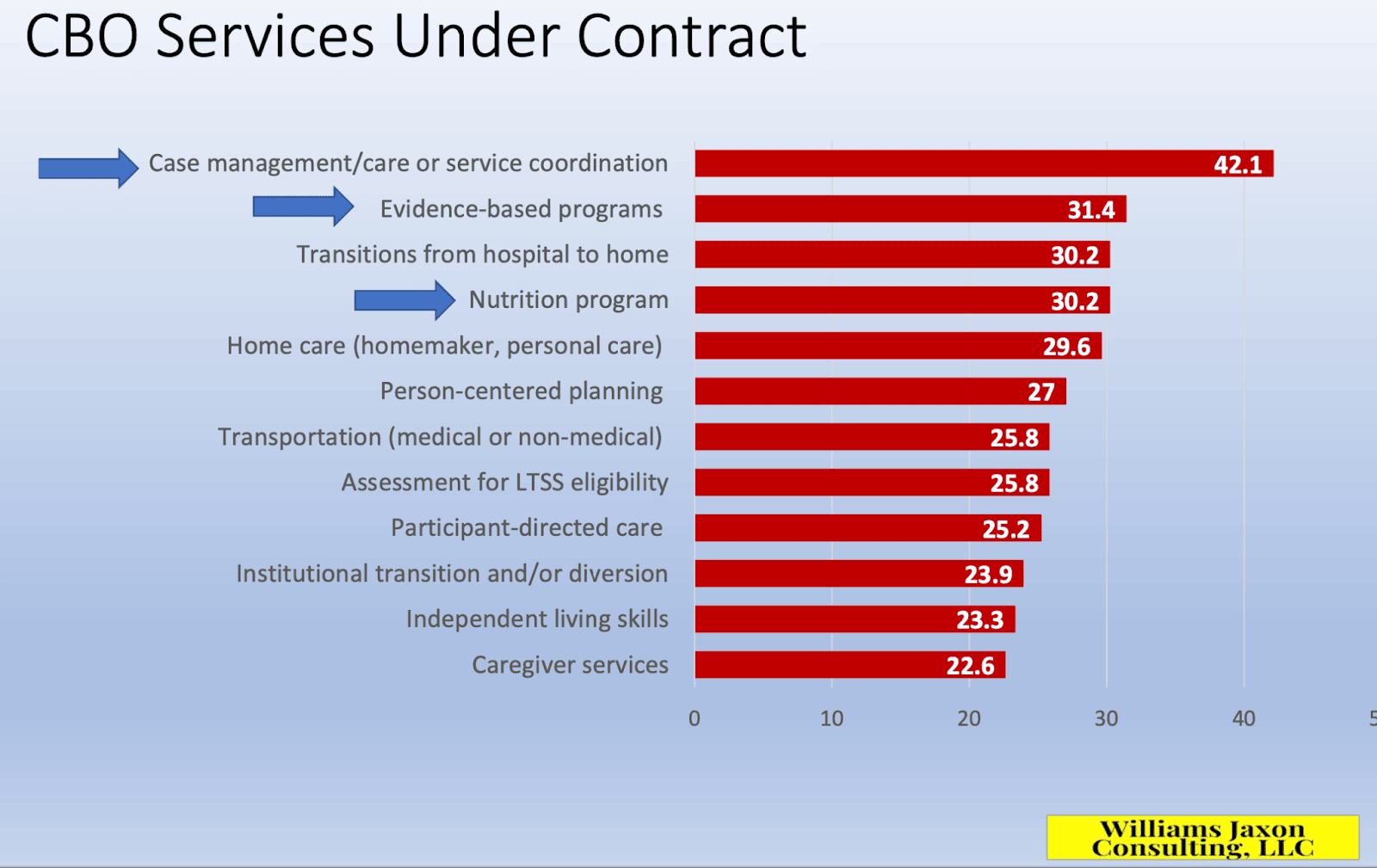
- Home and community based services (HCBS): As the chart below indicates, services like care coordination or care coordination offered through HCBS are some of the most likely areas for healthcare contracting currently.
Contractual engagement:
Can a CBO fulfill on the obligations of a contractual engagement? They might be looking at abilities a CBO has to perform services and not just do the work, but show the work through data and reporting.
- Compliance: Are your policies, procedures, and technology systems in place to comply with regulations like HIPAA or HITRUST?
- Network management and one-stop shopping: Do you have the reach to cover the necessary geographic areas to serve a plan or a provider’s members? Typically, healthcare wants to contract with the least number of entities possible to cover the network. It is much more attractive to work with a single CBO that can cover the whole network than to contract with a dozen different entities.
- Performance accountability: Many of the same expectations for healthcare providers are passed along to their contracted providers in terms of performance standards and service level agreements.
- Data integrity and reporting: This is a huge one. The level of rigor and sophistication required of data management is not to be underestimated. CBOs must be ready to meet a high standard of data collection and reporting requirements and should expect to provide real-time, accessible, verifiable data on service delivery and outcomes.
Conclusion
In future webinars and articles, we hope to explore further questions around how to prepare for contracting, how to start engaging healthcare, and how to manage those relationships.